During Holter reporting, I came across this ECG tracing.
My first thought was artefact, but the native rhythm which although irregular, has a regular pattern of irregularity!
What do you think?
I decided to review other tracings, particularly overnight, when the rhythm would be slow and the “artefact” less likely.
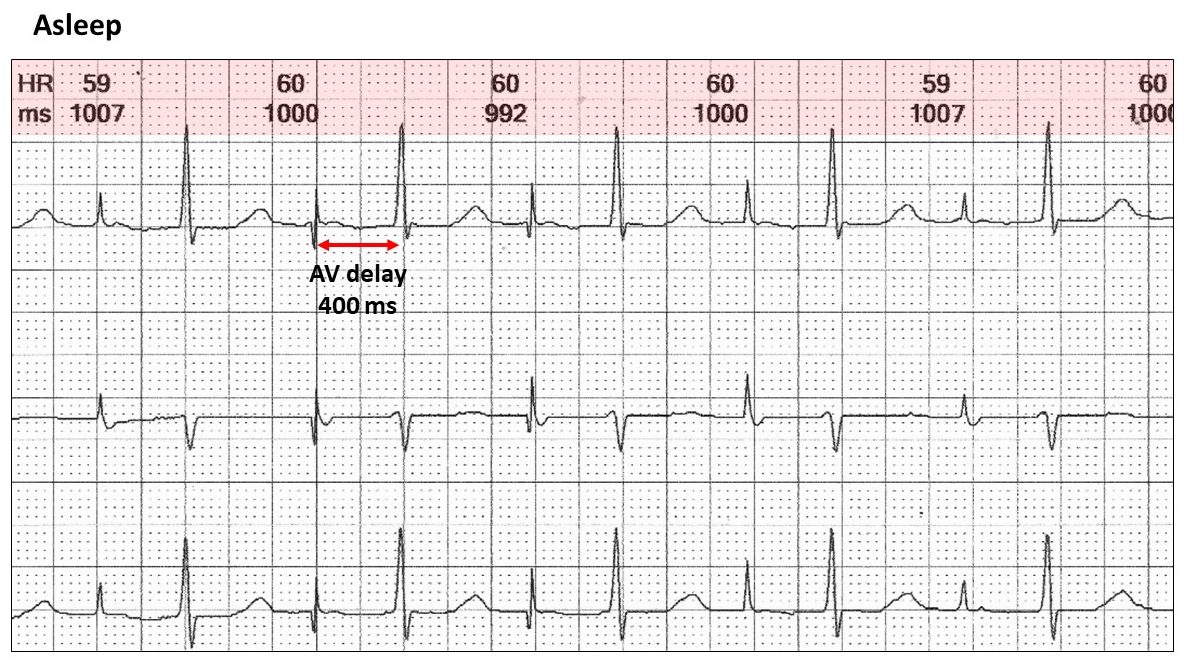
When asleep, the rhythm was exactly 60 bpm and clearly this is atrial pacing (AAIR) with a prolonged AV delay at rest of 400 ms. Because of double counting, the rate was stated to be 120 bpm all night. There was no ventricular pacing throughout the tracing.
Let us return to the original tracing.
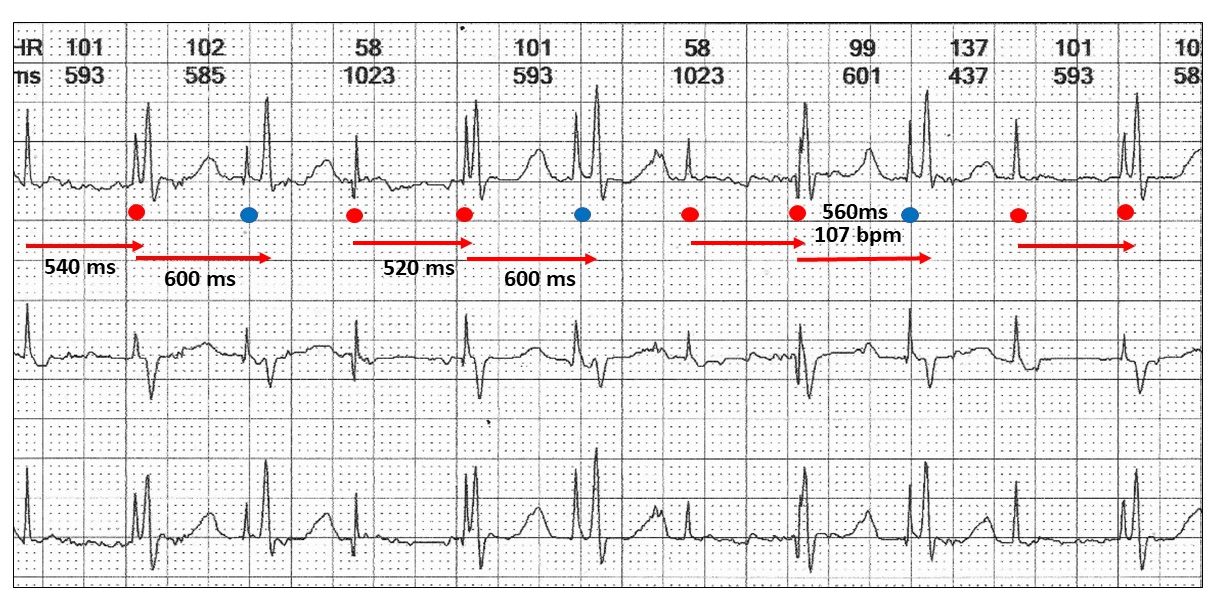
The atrial stimulus artefact rate is 107 bpm (560 ms) shown by the coloured dots.
Is there AV conduction?
There is a pattern with the AV delay now extending from 500 to 600 ms with 3:2 Wenckebach sequences. The blue dots are the dropped beats and occur before the conducted QRS.
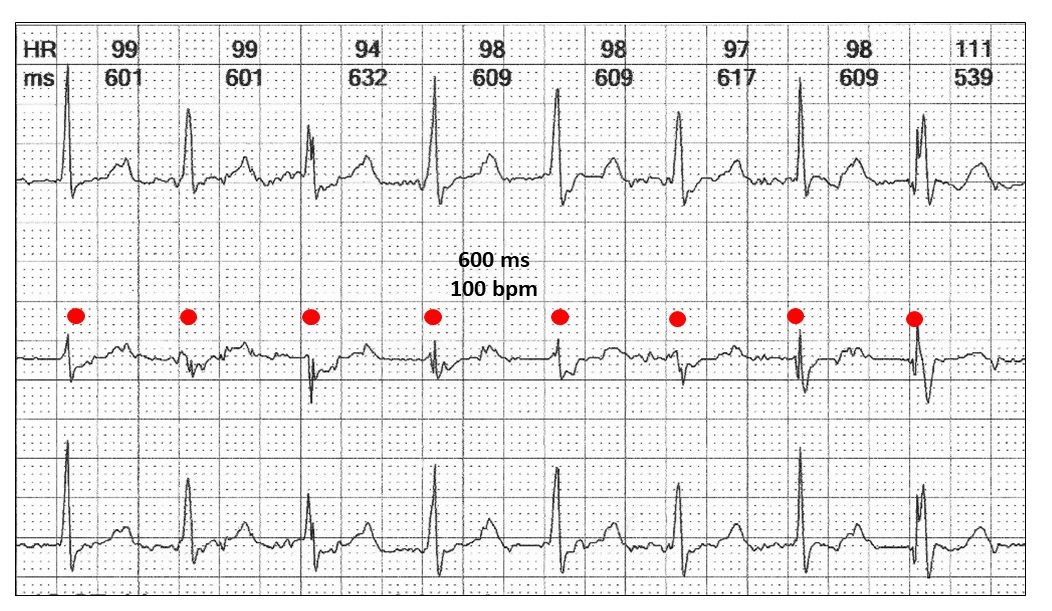
The next illustration shows a slightly slower heart rate of 100 bpm with 1:1 conduction resulting in a very confusing appearance.
The physiological consequences of atrial pacing within the native QRS means that atrial contraction occurs with closed AV valves; cannon waves in the neck and “pulsatile” pulmonary oedema known as the pacemaker syndrome. These patients are often very symptomatic with exertion. As they increase their atrial pacing rate, they feel they have run into a “brick wall”.
This is one of the major objections to single lead rate adaptive atrial pacing.
You may ask, could this be AAI pacing with a ventricular minimization pacing algorithm. The answer is no!! None of the manufacturer algorithms respond to repeated Wenckebach and very long AV delays without ventricular pacing. Also this cannot be DDD(R) pacing.
Programming of AAI(R) pacing in this situation is ridiculous!!
Here are some other examples:
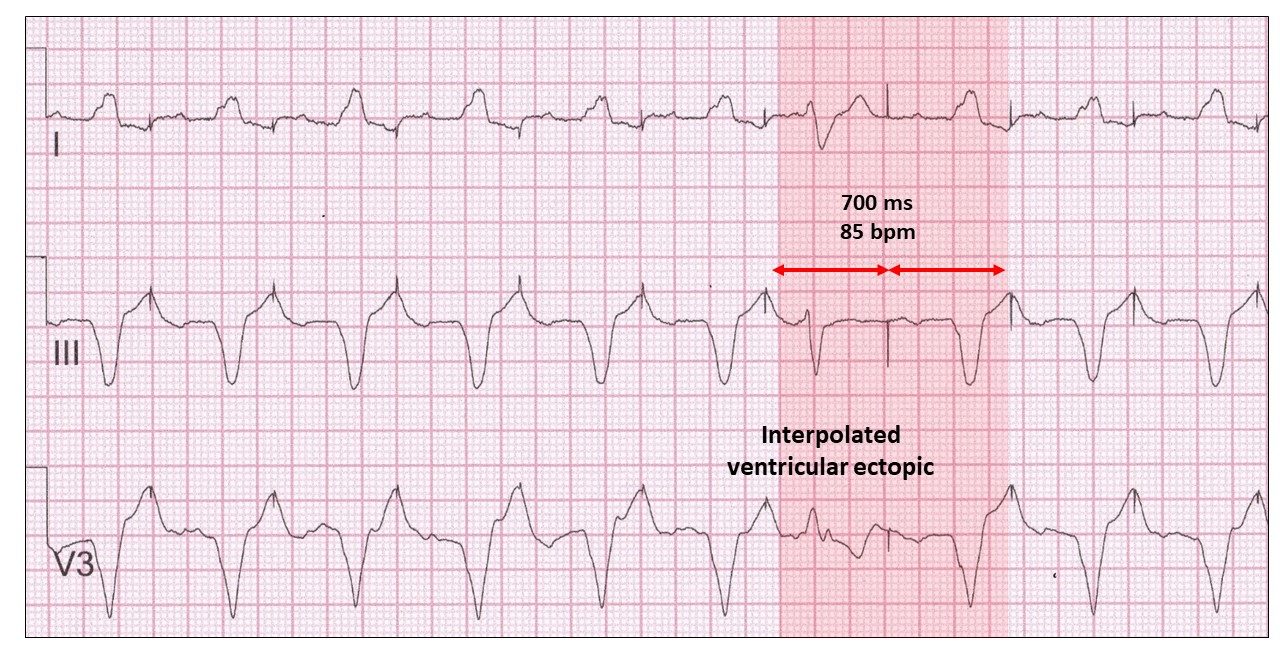
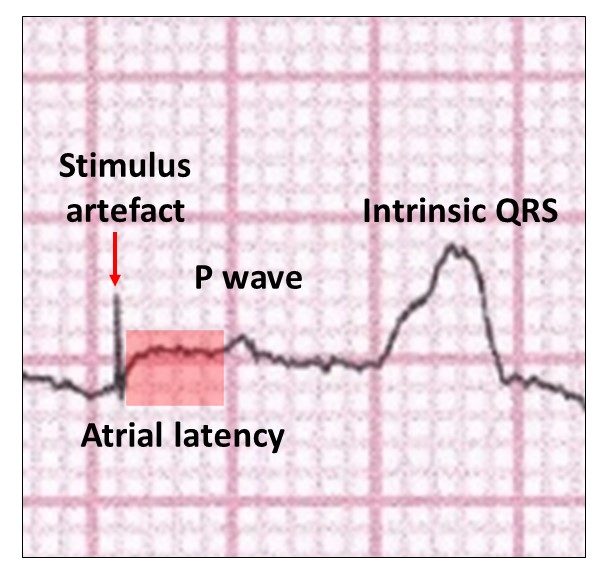
This is an interesting example at a relatively low atrial pacing rate of 85 bpm. There is an interpolated ventricular ectopic, which because of its prematurity allows the next atrial paced beat to fall beyond the T wave. Note the P wave in all leads commences late referred to as atrial latency and suggestive of severe atrial disease. Another name is “first degree pacemaker atrial block”. This means that atrial contraction is now physiologically appropriate, but with atrial disease may not be effective.
I have highlighted this in the next illustration.
Sometimes it gets silly!
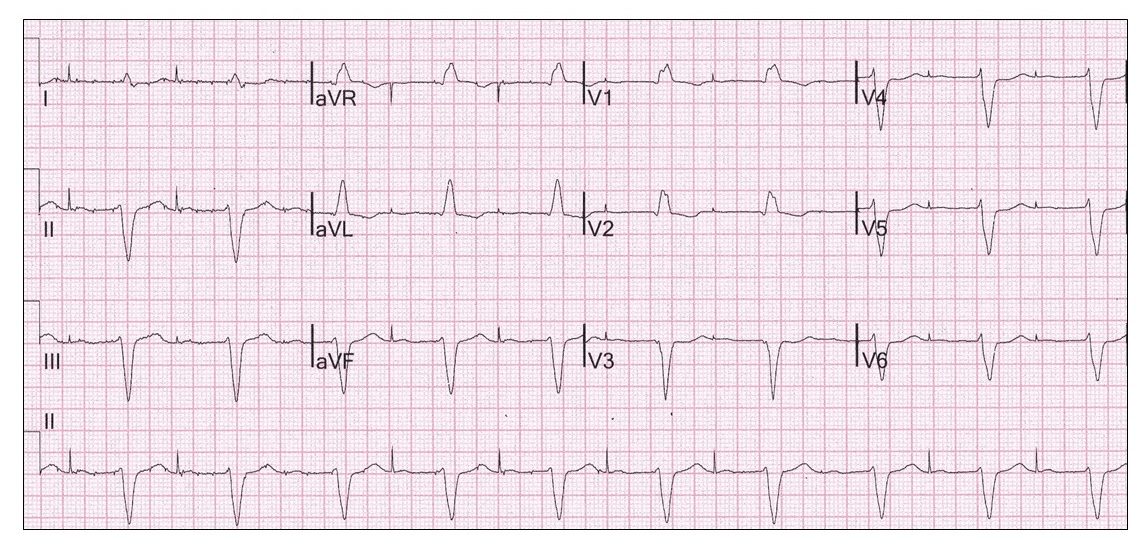
Even at rest it is obvious that AAI(R) pacing is innappropriate with marked first degree AV and bifascicular block. Irrespective of where the AV block in the conducting system lies, this form of pacing is not recommended.
Remember overnight Wenckebach at rest may be physiologic.
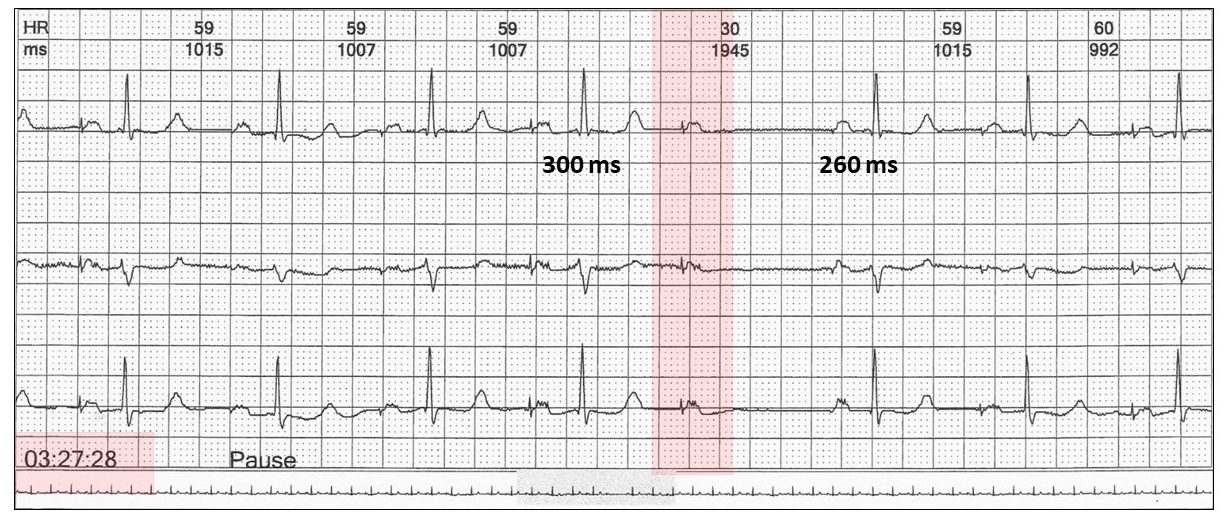
In this situation, the absence of conduction occurred only once and therefore may be innocent.
Harry Mond